How Can Ehr Be Efficient to a Family
Electronic Wellness Record Optimization and Clinician Well-Existence: A Potential Roadmap Toward Action
Baronial 3, 2020 | Discussion Newspaper


In the United States, 86 percent of office-based and 94 percent of hospital-based physicians currently utilise an electronic health record (EHR), incentivized by the 2009 Health Information Engineering for Economic and Clinical Health Human activity [1,2]. While intended to amend intendance quality and efficiency, the EHR has inadvertently burdened clinicians and is now considered a leading cause of their exhaustion [3,4,5]. Clinician burnout (a syndrome characterized by emotional exhaustion, depersonalization, and a depression sense of personal achievement) is associated with higher rates of medical errors, health intendance costs, and clinician turnover [6]. In Feb 2020, the Office of the National Coordinator for Wellness Data Technology published a strategy on reducing EHR-related burden, farther signaling the urgency for health intendance leaders to optimize the EHR [vii]. To shift the pendulum from clinician burnout to well-existence, it is imperative that health care organizations have activeness to optimize the EHR.
EHR optimization relies on human factors engineering, a scientific discipline that considers the benefits and fallibility of human interaction with a arrangement. Optimization requires a tailored, multipronged strategy that incorporates an organization's clinician-identified pain points, clinical information science and technology resources, and clinician and leadership buy-in. This paper provides strategies to help health care organizations embark on their EHR optimization journeying toward improved patient care and clinician well-being.
Problem Overview: Electronic Health Records and Clinician Well-Beingness
While EHRs take offered many benefits, EHR design currently emphasizes billing and administrative functions over care delivery and clinical decision making. Furthermore, archaic paper-based workflows were unremarkably transferred into electronic form instead of creating more streamlined, technology-enabled workflows. Clinicians spend half to 2-thirds of each workday on EHR and desk work instead of on direct patient care [8].
Indirectly, the EHR may disrupt the patient-clinician human relationship and increase inefficiencies, cognitive load, and the risk of clinician burnout. A focus on ensuring data elements for billing purposes are entered into the EHR has led to "note bloat," or excessively long notes. U.S. physicians' notes are 4 times every bit long equally their counterparts in other countries [9]. Many EHRs require an excessive number of steps, or clicks, to conduct out a simple office, such every bit reviewing a patient'southward allergies or renewing prescriptions. This phenomenon is then ubiquitous that it is known as "decease by a yard clicks" [10].
EHRs are often designed to ship alerts and messages about patient care tasks straight to the physician, regardless of the skill fix needed to process the tasks (e.g., medication refill requests, reminders to schedule cancer screenings, or obtaining test results). Consequently, the doc faces extra cognitive load from having to review or consummate patient care tasks that could exist delegated. A recent cess of physicians' in-basket messages, or EHR-based "east-post inbox" notifications, indicates that well-nigh half are auto-generated by the EHR and that clinicians are at twice equally much take chances for burnout when their inboxes included an above-average number of EHR-generated letters [11].
Optimizing the Electronic Health Tape: Strategies and Approaches to Address Well-Being
Fortunately, interventions are available that help accost clinician burnout associated with EHR utilise. Some of these strategies are available now, and others will be bachelor for future implementation—the proximity to implementation is noted underneath the championship of the intervention in each of the following sections.
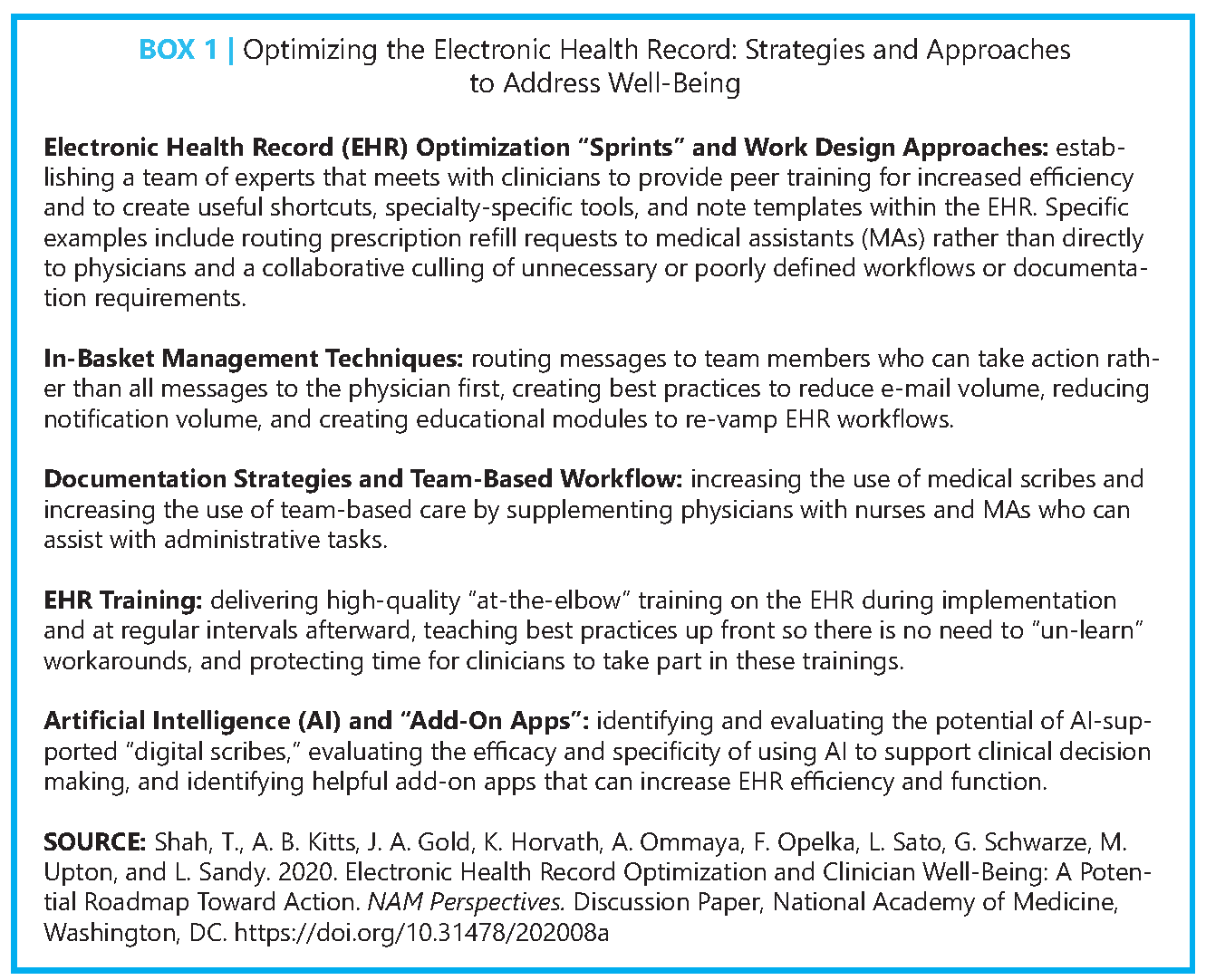
EHR Optimization "Sprints" and Work Pattern Approaches
Available Now
An EHR optimization "Dart" process (i.eastward., a short, intensive, team-based intervention) at the University of Colorado Wellness in Aurora, Colorado, significantly increased EHR satisfaction (e.g., Internet Promoter Score increased from –15 to +12) and reduced documentation time for clinicians [12]. The Dart team was composed of eleven staff members who carried out a 3-pronged intervention: (i) preparation clinicians to use the EHR more efficiently, (2) streamlining multidisciplinary clinic workflows, and (3) building new specialty-specific EHR tools. The squad met with clinical and part leaders 90, threescore, and thirty days prior to the Sprint to sympathise clinician pain points and current office workflows too as to create customized tools. Sprints lasted 5 to 20 days depending on the size of the practice and consisted of on-site kick-off meetings, i:1 observations and EHR efficiency training sessions, and deployment of new dispensary workflows using protected clinician time.
Erlanger Wellness System in Chattanooga, Tennessee, with assist from new EHR-based protocols, was able to increase the rate of paperwork completion and office visit documentation within ane twenty-four hours of the patient visit to 83 percent and reduce turnaround fourth dimension for medication refill authorizations to within i.2 days [13]. For medication refills, principal care (PC) physicians created EHR-based protocols to delegate processing these refills to registered nurses or medical administration (MAs). Importantly, the health system added additional personnel during EHR optimization to conduct listening sessions with EHR "super users," or actively practicing clinicians who can serve equally experts for their colleagues in the field, to ensure that pain points for actual workflows were addressed. Erlanger also tackled clinician-identified low- or no-value documentation requirements with insurers every bit office of broader efforts to reduce administrative EHR burden.
Hawaii Pacific Health in Honolulu, Hawaii, implemented an EHR entrada called "Getting Rid of Stupid Stuff," in which physicians and nurses across the organization were asked by senior leadership to nominate anything in the EHR that they felt was "poorly designed, unnecessary, or simply plain stupid" [14]. Co-ordinate to Ashton (2018), seventy-eight percent of the requests came from nurses, and almost nominations were about eliminating documentation that was not required by regulations or internal policies, improving efficiency of workflows, and creating ways to document more efficiently. More than half of the changes suggested had been completed or were in procedure past November 2018. While a formal assessment of impact on documentation burden or clinician burnout was non conducted, Ashton reported that the initiative was well received past employees.
Several other institutions—including Nemours Children'due south Wellness System, Oregon Health & Scientific discipline University, and Allina Health—are actively engaged in multipronged EHR optimization approaches likewise, which indicates that optimization is both immediately possible and highly of import to health systems and clinicians [15,xvi].
In-Handbasket Management Techniques
Available Now
Reliant Medical Group in Worcester, Massachusetts, rerouted sure types of in-basket letters to the appropriate clinical team members rather than sending all letters to physicians first, resulting in a 25 percent reduction in physician in-basket book [17]. Reliant also created guidelines for staff to reduce e-mail volume and ensure that eastward-mailed letters indicated a clear response or action needed for the recipient.
The Department of Veterans Affairs (VA) health system implemented a program to standardize and restrict EHR notifications to types on a recommended prove-based list and provided training to clinicians focused on customizing and processing notifications generated past the EHR. The program reduced the hateful number of daily notifications from 128 to 116 for each PC physician, which resulted in estimated fourth dimension savings of 1.v hours per week [xviii] and ancillary benefits on clinician well-being due to reduced notification and administrative burden, described earlier in this paper.
The American Medical Association (AMA) as well has an educational module containing a six-footstep plan to restructure EHR in-handbasket messages, relying on team-based care (TBC), in which a clinician is partnered with two to three MAs or nurses [19]. In addition to insights on how to achieve optimization by redirecting EHR messages to the right team member, this module provides guidance on using other TBC techniques to reduce a clinician's in-basket load, such as creating and utilizing a team in-basket that is accessed and worked on by multiple team members.
Documentation Strategies and Team-Based Workflow
Available At present
The use of medical scribes, or not-clinical staff who collect and enter data into EHRs in existent-time for the clinician, effectively reduces clinician time spent on documentation and provides other distinct advantages [20,21]. One written report using scribes in PC offices showed meaning improvements in md productivity and job satisfaction [22]. While potential disadvantages include the added expense of scribes, the frequency of scribe turnover, and associated grooming costs [23], these drawbacks can exist outset by an increase in clinician willingness and ability to run across more patients inside the same corporeality of time [24,25]. A few studies testify high patient credence of scribes [20,26,27]; however, this expanse needs further enquiry.
TBC is also a mechanism to address EHR inefficiencies. For case, a nurse and a md may acquit the in-person visit together, with the clinician focusing on the patient and the nurse assisting with documentation and orders [28]. In betwixt patient visits, clinical support staff process in-handbasket letters that take arisen during the day. At VA PC practices, a fully staffed care squad model was independently associated with lower clinician burnout (odds ratio 0.79) [29]. Additionally, VA PC practices with highly functioning TBC were found to be associated with lower staff burnout, college quality of clinical intendance, and higher patient satisfaction compared to practices with lower functioning TBC [xxx].
EHR Preparation
Available At present
Training clinicians on how to use the EHR, both during implementation and at regular intervals thereafter, is key to maximize efficiency and reduce the risk of burnout. In a survey of health care workers across 156 organizations, physicians that received poor preparation were 3.5 times more likely to written report that their EHR does not "enable them to evangelize high-quality care" [31]. Major barriers for training are a lack of protected time for clinicians, customized educational resources to roles and specialty, and consensus on metrics for exemplary (i.e., effective, efficient, and practiced) EHR use. Similar to other clinical skills, "at-the-elbow" preparation during protected time is perhaps more valuable to clinicians, as existent-time feedback can address unique needs alongside peer-to-peer learning.
Novice learners can be taught to apply best practices upfront instead of needing to "un-learn" ineffective behaviors. Training for learners should be multifaceted, with clear guidelines on roles and responsibilities for EHR-based work, provision of streamlined notation templates, and formal education to better note writing [32]. A widely accepted EHR training curriculum for students is needed but does not currently exist. The AMA launched a consortium of 32 medical schools to accelerate change in medical pedagogy, including an EHR training program that had more xix,000 participants as of 2018 [33]. Despite its significance for patient safe and clinician well-being, graduate medical training programs take neither focused on educational activity trainees how to excerpt or aggregate clinical information efficiently nor fully addressed the hidden agenda that fosters notation bloat from coding and billing inquiries.
Bogus Intelligence and "Improver Apps"
Only Down the Route
Apply of artificial intelligence (AI) tools such every bit natural language processing (NLP) and voice communication recognition (SR) to automate documentation are increasingly used in the health care sector [34]. NLP tin reliably extract data from free text sections in notes for billing purposes and create summaries to speed up a clinician's chart review [35]. SR software packages such as Dragon are commonly used to dictate into the EHR and accept been in use since 1994. A recent survey showed that 77 per centum of physicians who use SR stated that it improved efficiency [36].
Emerging technology chosen "digital scribes" seeks to combine SR, NLP, and other AI functionality to fully automate EHR-based documentation and work tasks (e.g., programs such as Suki and Nuance). Exam tools, such as an otoscope, tin too capture a variety of clinically useful data that can be straight digitized and transferred to the EHR. While these technologies are promising, they have yet to accurately capture all human interactions with patients (e.m., gesturing) and human-EHR interactions to obviate the need for a clinician to directly interact with the EHR. Furthermore, in that location are no sector-broad standards for this technology to ensure high quality in a real-world setting, so full integration of these tools into the clinical environment remains a futurity goal.
Across data capture and entry, AI volition be increasingly useful as a tool for clinical decision support. In imaging, AI algorithms have been developed and deployed to improve detection of lesions likely to be cancerous such equally from mammograms. Clinical utilization of these tools is currently variable and dependent on a range of factors, primarily due to concerns regarding generalizability, which tin can touch on clinician trust in predictive models [37].
One emerging application is "add together-on apps" that can seamlessly integrate with and enhance the functionality of EHRs. Fabricated possible by Health Level Seven International's Substitutable Medical Applications and Reusable Technologies (SMART) and Fast Healthcare Interoperability Resources (FHIR) standards, these apps, coined SMART-on-FHIR, have been successfully developed by both institutions and private industry, often to specifically aid in the direction of specific diseases or populations [38].
Electronic Wellness Record Optimization: Measurement and Governance
Measurement
Measurement of usability and subsequent optimization efforts should go on subsequently initial EHR deployment. Amongst other factors, EHRs should be evaluated for the following 3 aspects based on man factors engineering: (ane) their direct interface with the clinician, (ii) their bear on on unique workflows of the user'due south particular specialty, and (3) the physical environment in which they volition reside. User experience should also be measured specifically for satisfaction and burnout. A plan should also be developed for how selected metrics volition be validated for the specific user'due south intendance squad part, activity, specialty, and exercise setting.
Organizations should start with soliciting feedback from clinicians most which metrics they experience are most of import to monitor for EHR usability and EHR-related exhaustion. Every attempt should be made to apply existing and automatic data, including internal workplace and well-being surveys and vendor-provided metrics. Vendor-provided metrics include the number of mouse clicks and keystrokes to consummate a specific and isolated task [39,xl]; provider efficiency reports, which measure use of EHR-embedded efficiency tools such as order sets, macros, and hot keys, are besides useful [8,12]. "Pajama time," or after-hours EHR utilize, is straight correlated with clinician burnout and should be trended [8,41]. For in-basket monitoring, volume, types of messages being received, origin (i.eastward., arrangement- or provider-generated,) clinical value, and message processing time should be measured [42,43,44].
For additional needs, the Agency for Healthcare Research and Quality provides a compendium of validated wellness information technology (IT) tools [45]. Surveys that allow for external benchmarking such as the KLAS Curvation Collaborative survey, which has more than than 200 provider organization participants, should be considered [46]. Amidst multiple available survey tools for user satisfaction, a simple and well-validated approach is the System Usability Scale [47,48]. Eye-tracking and composite measures of workload, such equally the National Helmsmanship and Space Administration Task Load Index, can be helpful for measurement and to aid iterative workflow redesign [49].
Governance
The importance of health IT governance structures should not be overlooked to sustain EHR optimization. Smaller organizations may have an informal governance structure, while larger organizations may formalize a standing governance committee [50]. A standing governance committee should be multidisciplinary and include IT, finance, operational, and clinical leaders with representation across clinical sites of care. Big organizations ofttimes use a primary medical informatics officer (dr.), a chief nursing informatics officer (nurse), and/or a chief wellness information officer (with varied clinical or nonclinical background) to pb optimization work. Recently created roles such equally the chief wellness officeholder may too help in EHR optimization.
Clinical information science teams should exist established to provide readily available back up and to proactively seek out EHR challenges so that they tin be addressed before they become problematic [51]. These teams should include Information technology personnel and clinician super users who tin tackle specialty- and subject field-specific EHR nuances. A lack of medico informaticists or informatics staff resources are common reasons for EHR optimization failure and clinician burnout. While research is limited, studies suggest that a staffing ratio of 1 Information technology full-time equivalent (FTE) for every 50–lx non-IT FTEs is sufficient to back up EHR usability [52].
Designing for the Futurity: Emerging Technologies, Evaluation, and Implementation
There will need to be connected emphasis on user-centric EHR design, particularly as new applications extend legacy EHR platforms. As referenced above, AI and addon apps will continue to positively disrupt care delivery and should be embraced, rigorously tested, and deployed for use in the clinical setting.
Simulation is an ideal evaluation and testing method for new technologies or new technology applications in addition to improving EHR proficiency and efficiency [53]. Robust simulated patient records that are specialty and workflow congruent and contain enough information density and complexity to accurately assess efficacy for patient outcomes are key [53]. Simulation can also meliorate the preparation and onboarding plan for new users. In contrast to demonstration, simulation activities not simply effectively train the hereafter user on the new applied science merely too allow for rapid-cycle improvement for the grooming process.
Beyond EHRs, further advances in IT are on the horizon. One emerging direction is integration of aggregate information into a common data model from multiple sources (outside the EHR). Information from diverse sources can run through algorithms, which yield knowledge suited for individual use cases. EHRs will be a data entry betoken and a identify to receive AI for expression back to the patients and clinicians in real time at the moment of care. Withal, for these and others to follow, issues of bias, liability, and transparency (while beyond this newspaper'south scope) need to be addressed. Furthermore, information technology is essential that all technologies are tested and evaluated in the context of the providers using them and the surroundings in which they are used [54].
Conclusion
EHRs are a quintessential data platform for modern health care, nevertheless they possess major pattern and implementation challenges. Fortunately, there are many tools bachelor today to optimize EHRs for enhanced productivity, clinical intendance, and provider well-existence. Going forwards, additional best practices demand to be developed, and future generations of EHRs and other health IT tools need to be designed with human factors engineering science principles to ensure a focus on usability. Strategies in use and/or under development include:
- engaging clinicians often in the initial stages of EHR implementation and during evaluation and optimization of EHR usability,
- implementing peer-led training programs and periodically training clinicians to improve EHR efficiency after initial deployment,
- focusing on workflow redesign as part of EHR optimization,
- implementing TBC models and including ancillary staff such as scribes,
- developing strategies and governance to reduce low-value in-basket letters and limit other notifications, and
- investing in man factors assessment of the piece of work environment to ensure that "right person, correct place, right time" is adhered to for all wellness care workers.
Join the conversation!
![]() Tweet this! While meant to meliorate care quality and efficiency, the EHR has inadvertently burdened clinicians. A new #NAMPerspectives outlines interventions available now that can move the EHR toward supporting #ClinicianWellBeing: https://doi.org/10.31478/202008a
Tweet this! While meant to meliorate care quality and efficiency, the EHR has inadvertently burdened clinicians. A new #NAMPerspectives outlines interventions available now that can move the EHR toward supporting #ClinicianWellBeing: https://doi.org/10.31478/202008a
![]() Tweet this!Only implementing targeted, tailored training on the EHR can contribute significantly to its efficiency and effectiveness in the clinical workplace. A new #NAMPerspectives examines this intervention and more: https://doi.org/10.31478/202008a #ClinicianWellBeing
Tweet this!Only implementing targeted, tailored training on the EHR can contribute significantly to its efficiency and effectiveness in the clinical workplace. A new #NAMPerspectives examines this intervention and more: https://doi.org/10.31478/202008a #ClinicianWellBeing
![]() Tweet this!#AI and machine learning may be able to be leveraged in the near hereafter to ensure that the EHR contributes to #ClinicianWellBeing. Read a new #NAMPerspectives to hear nigh this and other interventions available just down the road: https://doi.org/10.31478/202008a
Tweet this!#AI and machine learning may be able to be leveraged in the near hereafter to ensure that the EHR contributes to #ClinicianWellBeing. Read a new #NAMPerspectives to hear nigh this and other interventions available just down the road: https://doi.org/10.31478/202008a
Download the graphics below and share them on social media!
References
- Myrick, 1000. L., D. F. Ogburn, and B. W. Ward. 2019. Percentage of office-based physicians using any electronic health tape (EHR)/electronic medical tape (EMR) system and physicians that have a certified EHR/EMR system, by U.S. country: National Electronic Wellness Records Survey, 2017. National Center for Health Statistics. Bachelor at: https://world wide web.cdc.gov/nchs/data/nehrs/2017_NEHRS_Web_Table_EHR_State.pdf (accessed June 1, 2020).
- Office of the National Coordinator for Health Information Technology. 2019. Hospitals' use of electronic health records data, 2015–2017. ONC Data Brief No. 46. Available at: https://www.healthit.gov/sites/default/files/page/2019-04/AHAEHRUseData-Brief.pdf (accessed June one, 2020).
- Friedberg, M. W., P. 1000. Chen, Yard. R. Van Busum, F. Aunon, C. Pham, J. P. Caloyeras, South. Mattke, E. Pitchforth, D. D. Quigley, R. H. Brook, F. J. Crosson, and M. Tutty. 2013. Factors affecting dr. professional satisfaction and their implications for patient care, health systems, and health policy. Santa Monica, CA: RAND Corporation. Available at: https://pubmed.ncbi.nlm.nih.gov/28083306 (accessed June one, 2020).
- Shanafelt, T. D., 50. North. Dyrbye, C. Sinsky, O. Hasan, D. Satele, J. Sloan, and C. P. West. 2016. Human relationship between clerical brunt and characteristics of the electronic environment with dr. exhaustion and professional satisfaction. Mayo Clinic Proceedings 91(7):836–848. https://doi.org/ 10.1016/j.mayocp.2016.05.007.
- Stanford Medicine. 2018. How doctors feel nearly electronic wellness records: National medico poll. The Harris Poll. Available at: http://www.med.stanford.edu/content/dam/sm/ehr/documents/EHR-Poll-Presentation.pdf (accessed February 28, 2020).
- Dyrbye, 50. N., T. D. Shanafelt, C. A. Sinsky, P. F. Cipriano, J. Bhatt, A. Ommaya, C. P. West, and D. Meyers. 2017. Burnout amid health care professionals: A phone call to explore and address this underrecognized threat to prophylactic, high-quality intendance. NAM Perspectives. Give-and-take Paper, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/201707b.
- The Role of the National Coordinator for Health Information Applied science. 2020. Strategy on reducing regulatory and administrative brunt relating to the utilize of wellness It and EHRs. Bachelor at: https://www.healthit.gov/sites/default/fi les/webform/reducing_burden_report/draft-strategy-on-reducing-regulatory-and-administrative-burden-relating—rkb-comments.pdf (accessed March 10, 2020).
- Arndt, B. Chiliad., J. W. Beasley, M. D. Watkinson, J. Fifty. Temte, W. Tuan, C. A. Sinsky, and V. J. Gilchrist. 2017. Tethered to the EHR: PC doc workload assessment using EHR event log data and time-movement observations. Annals of Family Medicine 15(5):419–426. https://doi.org/10.1370/afm.2121.
- Downing, N. L., D. W. Bates, and C. A. Longhurst. 2018. Doctor exhaustion in the electronic health tape era: Are we ignoring the real crusade? Annals of Internal Medicine 169:50–51. https://doi.org/10.7326/M18-0139.
- Schulte, F., and E. Fry. 2019. Death past a m clicks: Where electronic wellness records went incorrect. Kaiser Health News. Available at: https://www.healthleadersmedia.com/innovation/deaththousand-clicks-where-electronic-health-recordswent-incorrect (accessed May thirteen, 2020).
- Tai-Seale, 1000., E. C. Dillon, Y. Yang, R. Nordgren, R. Fifty. Steinberg, T. Nauenberg, T. C. Lee, A. Meehan, J. Li, A. Southward. Chan, and D. L. Frosch. 2019. Physicians' well-beingness linked to in-basket messages generated by algorithms in electronic wellness records. Wellness Affairs 38(7):1073–1078. https://doi.org/x.1377/hlthaff .2018.05509.
- Sieja, A., K. Markley, J. Pell, C. Gonzalez, B. Redig, P. Kneeland, and C. Lin. 2019. Optimization Sprints: Improving clinician satisfaction and teamwork by chop-chop reducing electronic health record burden. Mayo Clinic Proceedings 94(5):793–802. https://doi.org/10.1016/j.mayocp.2018.08.036.
- American Hospital Association Physician Alliance. 2018. Erlanger Health Organisation. Available at: https://www.aha.org/organization/files/2018-11/plf-example-studyerlanger.pdf (accessed Feb 28, 2020).
- Ashton, K. 2018. Getting rid of stupid stuff. New England Journal of Medicine eight(19):1789–1791. https://doi.org/10.1056/NEJMp1809698.
- Raths, D. 2019. With physician burnout rising, EHR optimization takes middle stage. Healthcare Innovation. Available at: https://www.hcinnovationgroup.com/clinical-it/article/21089517/with-physicianburnout-rising-ehr-optimization-takes-centerstage (accessed February 28, 2020).
- American Hospital Association. 2020. Exist well case studies. Available at: https://world wide web.aha.org/exist-wellcase-studies (accessed March ten, 2020).
- Massachusetts Medical Order. 2019. Changing the EHR from a liability to an asset to reduce doc burnout: The Reliant Medical Group story. Available at: http://www.massmed.org/News-and-Publications/Changing-EHR-Physician-Burnout (accessed February 28, 2020).
- Shah, T., Southward. Patel-Teague, L. Kroupa, A. Meyer, and H. Singh. 2019. Touch on of a national QI programme on reducing electronic health record notifications to clinicians. BMJ Quality and Rubber 28(1):x–14. https://doi.org/10.1136/bmjqs-2017-007447.
- Jerzak, J., and C. Sinsky. 2017. EHR in-handbasket restructuring for improved efficiency. American Medical Association Steps Forrad. Available at: https://edhub.ama-assn.org/steps-forwards/module/2702694 (accessed May 13, 2020).
- Gidwani, R., C. Nguyen, A. Kofoed, C. Carragee, T. Rydel, I. Nelligan, A. Sattler, M. Mahoney, and S. Lin. 2017. Bear upon of scribes on medico satisfaction, patient satisfaction, and charting efficiency: A randomized controlled trial. Annals of Family Medicine 15(five):427–433. https://doi.org/ten.1370/afm.2122.
- Smith, C. D., C. Balatbat, Due south. Corbridge, A. L. Dopp, J. Fried, R. Harter, S. Landefeld, C. Martin, F. Opelka, L. Sandy, 50. Sato, and C. Sinsky. 2018. Implementing optimal team-based care to reduce clinician burnout. NAM Perspectives. Discussion Paper, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/201809c.
- Mishra, P., J. C. Kiang, and R. W. Grant. 2018. Clan of medical scribes in PC with physician workflow and patient experience. JAMA Internal Medicine 178(eleven):1467–1472. https://doi.org/ten.1001/jamainternmed.2018.3956.
- Williams, Chiliad. 2016. The pros and cons of using scribes. ACP Internist. Bachelor at: https://acpinternist.org/athenaeum/2016/10/tips.htm (accessed June one, 2020).
- Bank, A. J., C. Obetz, A. Konrardy, A. Khan, 1000. M. Pillai, B. J. McKinley, R. 1000. Gage, 1000. A. Turnbull, and Due west. O. Kenney. 2013. Impact of scribes on patient interaction, productivity, and revenue in a cardiology clinic: A prospective study. ClinicoEconomics and Outcomes Research five:399–406. https://doi.org/10.2147/ceor.s49010.
- Nambudiri, 5. E., A. J. Watson, E. A. Buzney, T. Due south. Kupper, Thou. H. Rubenstein, and F. C. Yang. 2018. Medical scribes in an academic dermatology practise. JAMA Dermatology 54(1):101–103. https://doi.org/10.1001/jamadermatol.2017.3658.
- Pozdnyakova, A., N. Laiteerapong, A. Volerman, L. D. Feld, W. Wan, D. Fifty. Burnet, and Westward. W. Lee. 2018. Impact of medical scribes on physician and patient satisfaction in principal care. Journal of Full general Internal Medicine 33(7):1109–1115. https://doi.org/x.1007/s11606-018-4434-6.
- Zallman, L., One thousand. Finnegan, D. Coil, M. Todaro, R. Oneiz, and A. Sayah. 2018. Impact of medical scribes in PC on productivity, confront-to-face time, and patient comfort. Journal of the American Lath of Family unit Medicine 7(1):612–619. https://doi.org/10.3122/jabfm.2018.04.170325.
- Sinsky, C. A., and T. Bodenheimer. 2019. Powering-upward primary care teams: Avant-garde team care with in-room support. Annals of Family unit Medicine 17(4):367–371. https://doi.org/10.1370/afm.2422.
- Helfrich, C. D., E. D. Dolan, J. Simonetti, R. J. Reid, S. Joos, B. J. Wakefield, Thou. Schectman, R. Stark, Due south. D. Fihn, H. B. Harvey, and K. Nelson. 2014. Elements of team-based intendance in a patient-centered medical home are associated with lower burnout among VA main care employees. Journal of General Internal Medicine 29:659–666. https://doi.org/10.1007/s11606-013-2702-z.
- Nelson, K. M., C. Helfrich, H. Sun, P. Fifty. Hebert, C. F. Liu, E. Dolan, L. Taylor, E. Wong, C. Maynard, Due south. Eastward. Hernandez, W. Sanders, I. Randall, I. Curtis, Yard. Schectman, R. Stark, and Southward. D. Fihn. 2014. Implementation of the patient-centered medical domicile in the Veterans Wellness Administration: Associations with patient satisfaction, quality of care, staff exhaustion, and infirmary and emergency section use. JAMA Internal Medicine 174(viii):1350–1358. https://doi.org/10.1001/jamainternmed.2014.2488.
- Longhurst, C. A., T. Davis, A. Maneker, H. C. Eschenroeder Jr., R. Dunscombe, G. Reynolds, B. Clay, T. Moran, D. B. Graham, S. M. Dean, and J. Adler-Milstein. 2019. Local investment in grooming drives electronic wellness record user satisfaction. Applied Clinical Information science 10(two):331–335. https://doi.org/ten.1055/s-0039-1688753.
- Dean, South. G., J. C. Eickhoff , and L. A. Bakel. 2015. Improving notes in the EHR. Periodical of Infirmary Medicine 2:104–107. https://doi.org/10.1002/jhm.2283.
- Monica, K. 2018. AMA expanding EHR training, medical education consortium. EHR Intelligence. Bachelor at: https://ehrintelligence.com/news/ama-expanding-ehr-training-medical-educationconsortium (accessed March 10, 2020).
- Coiera, E., B. Kocaballi, J. Halamka, and L. Laranjo. 2018. The digital scribe. NPJ Digital Medicine 1:58. https://doi.org/10.1038/s41746-018-0066-ix.
- Ommaya, A. K., P. F. Cipriano, D. B. Hoyt, K. A. Horvath, P. Tang, H. L. Paz, M. S. DeFrancesco, S. T. Hingle, S. Butler, and C. A. Sinsky. 2018. Care-centered clinical documentation in the digital surroundings: Solutions to alleviate burnout. NAM Perspectives. Discussion Newspaper, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/201801c.
- Goss, F. R., Southward. V. Blackley, C. A. Ortega, Fifty. T. Kowalski, A. B. Landman, C. T. Lin, K. Meteer, Due south. Bakes, S. C. Gradwohl, D. Westward. Bates, and 50. Zhou. 2019. A clinician survey of using speech recognition for clinical documentation in the electronic wellness record. International Journal of Medical Informatics 130. https://doi.org/ten.1016/j.ijmedinf.2019.07.017.
- Kelly, C. J., A. Karthikesalingam, M. Suleyman, G. Corrado, and D. King. 2019. Cardinal challenges for delivering clinical impact with artificial intelligence. BMC Medicine 17:195. https://doi.org/10.1186/s12916-019-1426-two.
- Kawamoto, K., P. Kukhareva, J. H. Shakib, H. Kramer, S. Rodriguez, P. B. Warner, D. Shields, C. Weir, G. Del Fiol, T. Taft, and C. H. Stipelman. 2019. Association of an Electronic Wellness Tape add-on app for neonatal bilirubin management with doctor efficiency and intendance quality. JAMA Network Open 2(11):e1915343. https://doi.org/ten.1001/jamanetworkopen.2019.15343.
- Ratwani, R. M., E. Roughshod, A. Will, A. Fong, D. Karavite, N. Muthu, A. J. Rivera, C. Gibson, D. Asmonga, B. Moscovitch. R. Grundmeier, and J. Rising. 2018. Identifying electronic wellness tape usability and condom challenges in pediatric settings. Health Affairs 37(11):1752–1759. https://doi.org/ 10.1377/hlthaff .2018.0699.
- Gold, J. A., L. E. Stephenson, A. Gorsuch, Grand. Parthasarathy, and V. Mohan. 2015. Feasibility of utilizing a commercial eye tracker to assess electronic health record apply during patient simulation. Health Computer science Journal 22(iii):744–757. https://doi.org/10.1177/1460458215590250.
- Gardner, R. L., E. Cooper, J. Haskell, D. A. Harris, S. Poplau, P. J. Kroth, and G. Linzer. 2019. Dr. stress and exhaustion: The impact of health it. Journal of the American Medical Informatics Clan 26(2):106–114. https://doi.org/x.1093/jamia/ocy145.
- Kizzier-Carnahan, V., K. A. Artis, V. Mohan, and J. A. Gold. 2019. Frequency of passive EHR alerts in the ICU: Another form of warning fatigue? Journal of Patient Rubber 15(3):246–250. https://doi.org/ten.1097/PTS.0000000000000270.
- Lin, C. P., T. H. Payne, W. P. Nichol, P. J. Hoey, C. L. Anderson, and J. H. Gennari. 2008. Evaluating clinical determination support systems: Monitoring CPOE social club bank check override rates in the Department of Veterans Affairs' computerized patient record system. Journal of the American Medical Informatics Association 15(5):620–626. https://doi.org/10.1197/jamia.M2453.
- Spirk, D., A. K. Stuck, A. Hager, R. P. Engelberger, D. Aujesky, and N. Kucher. 2017. Electronic alert organization for improving advisable thromboprophylaxis in hospitalized medical patients: A randomized controlled trial. Journal of Thrombosis and Haemostasis 15(11):2138–2146. https://doi.org/ten.1111/jth.13812.
- Digital Healthcare Inquiry. 2020. Wellness It survey compendium. Agency for Healthcare Inquiry and Quality. Available at: https://digital.ahrq.gov/wellness-it-tools-and-resources/evaluation-resource/health-information technology-survey-compendium-search (accessed March 10, 2020).
- KLAS. 2020. Domicile. Available at: https://klasresearch.com/dwelling (accessed March x, 2020).
- Brooke, J. 1996. SUS: A "quick and dirty" usability scale. In Usability evaluation in industry, edited by P. W. Hashemite kingdom of jordan, B. Thomas, B. A. Weerdmeester, and I. 50. McClelland, pp. 189–194. London: Taylor & Francis.
- Sandefer, R., D. Brinda, J. Wapola, S. East. Maki, and D. Marc. 2013. EHR usability on mobile devices. Educational Perspectives in Health Informatics and Data Management 1–11. Available at: https://pdfs.semanticscholar.org/09e3/ae0769cf0c9b7e32d69550c4846aafe472bf.pdf?_ga=2.22700091.1287485016.1591114417-1171844949.1589903450 (accessed June 2, 2020).
- Hart, South. Yard. 2006. Nasa-Task Load Index (NASA-TLX); xx Years Later on. Proceedings of the Human Factors and Ergonomics Society Almanac Meeting fifty:904–908. https://doi.org/x.1177/154193120605000909.
- The Part of the National Coordinator for Health It. 2020. Data Governance. Available at: https://world wide web.healthhit.gov/playbook/ambulatory-guide/information-governance (accessed March 10, 2020).
- Rajaram, A., H. Zachary, P. Nimesh, North. Joseph, and B. Wolfrom. 2020. Training medical students and residents in the utilize of electronic health records: A systematic review of the literature. Journal of the American Medical Informatics Clan 27(1):175–180. https://doi.org/10.1093/jamia/ocz178.
- Hersh, W. 2010. The health information technology workforce: Estimations of demands and a framework for requirements. Applied Clinical Informatics 1(2):197–212. https://doi.org/10.4338/ACI-2009-11-R-0011.
- Mohan, V., D. Woodcock, K. McGrath, G. Scholl, R. Pranaat, J. W. Doberne, D. A. Chase, J. A. Gold, and J. Southward. Ash. 2016. Using simulations to meliorate electronic health tape apply, clinician preparation and patient safety: Recommendations from a consensus conference. AMIA Annual Symposium Proceedings Archive 904–913. Bachelor at: https://pubmed.ncbi.nlm.nih.gov/28269887 (accessed June ii, 2020).
- Takeuchi, Westward., S. Tarumi, Southward. Rodriquez, D. Shields, P. Warner, M. Flynn, K. Turner, F. Sakaguchi, H. Ban, and K. Kawamoto. 2018. EHR-integrated, machine learning-driven SMART on FHIR pharmacotherapy decision back up arrangement for type-2 diabetes mellitus. Newspaper presented at the AMIA 2018 Computer science Meridian, San Francisco, CA. Available at: https://noesis.amia.org/amia-66728-cri2018-one.4079151/t004-i.4080149/f004-1.4080150/a090-i.4080157/an090-1.4080158?qr=ane (accessed June 2, 2020).
Source: https://nam.edu/electronic-health-record-optimization-and-clinician-well-being-a-potential-roadmap-toward-action/
0 Response to "How Can Ehr Be Efficient to a Family"
Post a Comment